The Hormone-Brain Connection: What Every Woman Over 40 Should Know
By Dr. Sarah Ellison, MD · 6 min read · April 23, 2026
You walk into a room and forget why you're there. You lose a word mid-sentence -- a word you've used a thousand times. You finish a meeting and realize you retained almost nothing. You wonder, quietly, if something is wrong with you.
You're not alone, and nothing is wrong with you. What's happening is hormonal. And the research on exactly how is finally catching up.
Estrogen Is a Brain Chemical, Not Just a Reproductive One
Most women understand estrogen in terms of their cycle: it rises before ovulation, drops before menstruation, and declines as they approach menopause. What fewer women are told is that estrogen is also a potent neuroactive hormone -- one that directly shapes how the brain functions.
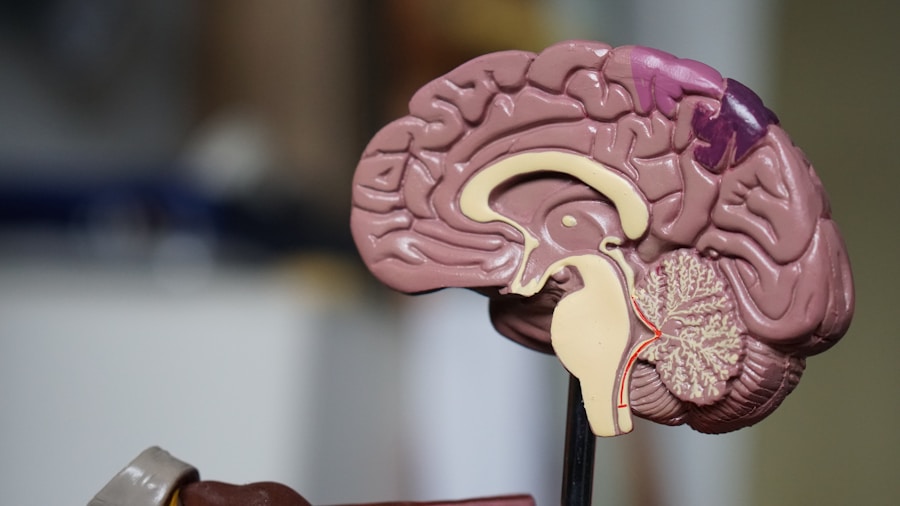
Estrogen receptors are found throughout the central nervous system. They are concentrated in the hippocampus (the region responsible for memory consolidation), the prefrontal cortex (involved in decision-making and executive function), and the limbic system (which governs mood and emotional processing).
This means that when estrogen levels fluctuate -- as they do throughout perimenopause -- the effects are not limited to the body. They ripple through the brain.
What Happens to Cognition During Perimenopause
Research published in journals including Neurology and Menopause has documented a consistent pattern of cognitive changes in perimenopausal women:
Verbal memory (the ability to recall words and names) is among the first areas to show decline.
Processing speed -- how quickly the brain handles new information -- slows noticeably in early perimenopause.
Working memory (holding information in mind while using it) becomes less reliable.
Attention and concentration fluctuate, often correlating with sleep quality and estrogen variability.
These changes are real, measurable, and documented. They are not "just stress." They are not a personal failing. They are a physiological response to declining neuroactive hormone levels.
The Sleep-Cognition Loop
One of the more insidious aspects of perimenopausal cognitive change is how closely it is tied to sleep disruption. Estrogen and progesterone both play roles in regulating sleep architecture -- particularly the deep, slow-wave sleep that is essential for memory consolidation.
When these hormones fluctuate, sleep suffers. And when sleep suffers, cognition suffers in turn.
This creates what researchers sometimes call the "sleep-cognition loop": hormonal changes disrupt sleep, poor sleep accelerates cognitive symptoms, and the resulting fatigue and brain fog feel indistinguishable from one another.
Why This Matters for How You Approach Treatment
Understanding the sleep-cognition link changes what "addressing brain fog" actually means. Targeting cognitive symptoms in isolation -- with caffeine, mental exercises, or single-purpose nootropics -- misses the upstream hormonal mechanism driving them.
The same is true of addressing only hot flashes, or only sleep. In perimenopause, symptoms are rarely isolated. They share a root.
What the Research Says About Support
The clinical literature on cognitive function in perimenopause points consistently toward multi-pathway support: approaches that address hormonal balance, sleep quality, and neuroinflammation together, rather than in sequence.
Several well-studied botanical actives have demonstrated effects on estrogen receptor activity in the brain. Others have shown measurable improvements in verbal memory and processing speed in perimenopausal populations. A growing body of research also supports the role of adaptogenic compounds in modulating the HPA axis response to hormonal stress -- which directly influences cognitive load and mental clarity.
What this means practically: the most effective support for perimenopause-related brain fog is not a single ingredient. It is a comprehensive formula targeting the interconnected systems involved.
When to Take Cognitive Symptoms Seriously
Not every moment of forgetfulness is a perimenopause symptom. But if you are noticing a pattern -- consistent word retrieval difficulty, trouble concentrating that interferes with work, a sense of mental "fog" that doesn't lift after sleep -- it is worth taking seriously.
First, rule out other contributors: thyroid dysfunction, anemia, vitamin D deficiency, and certain medications can all affect cognition. A conversation with your physician is always the right starting point.
If hormonal changes are the driver, addressing them early tends to produce better outcomes. Research suggests that cognitive function is more responsive to hormonal support during the early perimenopausal transition than after menopause has been established for several years.
The implication: if you're noticing changes now, the best time to act is now.
The Bigger Picture
Perimenopause is often framed as a reproductive transition. It is also a neurological one. The brain you have at 50 is shaped, in part, by how well you support your hormonal health during the transition years.
That doesn't mean cognitive changes are inevitable or permanent. Many women report significant improvement in mental clarity when they address the hormonal and sleep foundations that underlie it. The research supports this. And the window for that support is most effective earlier, not later.
If you're not sure where you are in your transition or what kind of support fits your profile, our 3-minute quiz can help you identify the right approach for your specific symptoms and stage.
The information in this article is for educational purposes only and does not constitute medical advice. Consult your healthcare provider for guidance specific to your health situation.